Why?
Our family’s choice not to participate in the COVID-19 vaccination
(data collected 9/30/21, version 10/16/21)
“Why are you choosing to not receive a COVID-19 vaccine?” This is a common question being asked by our friends, family, and physicians these days who genuinely care about our health and well-being. And we (my wife and I) sincerely appreciate that concern. This simple question has a complex answer that a 15-minute conversation does not afford. This document is certainly not exhaustive, but it is intended to help communicate the reasons “Why” using data, people’s own words, medical journals, and mainstream news sources.
All of the information used to guide us to our conclusion will be linked. Please do not simply take our word for any of this, review the referenced source material! We hope this stimulates you to do your own research (if you are doing searches on the internet, be aware of censorship and AI algorithms that shape the search results, not all search engines are the same), and do something dangerous… think critically, even when you are told not to.
There was a study released by Carnegie Mellon University about COVID vaccine hesitancy in July of 2021. After quiet introspection, I admittedly fit nearly all the risk factors described (besides the ≤ high school education).
“Trust the Science” is a well-used moniker these days. I have a Bachelor’s of Science degree in Engineering. I spent more than my fair share of time in the lab. Yet, I think we should all be able to answer these elementary questions:
Q: What is science?
A: The study of our physical world.
Q: How does one study our physical world?
A: The scientific method is a good approach to do this.
Q: What is the scientific method?
A: 1) Identify a Problem/Question 2) Form a Hypothesis 3) Experiment 4) Observe and Record 5) Analyze Then Make a Conclusion or Refine and Repeat
Let us participate in a scientific method exercise. First step:
1) Problem
As described in a recent story (9/15/21) by the Washington Post — 1 in 500 Americans have died from COVID
Let us look at their numbers a little closer:

Let us now convert those figures to percentages:
1/35 = 2.86% of the pop over 85 (point of ref: 1 in 27 odds of death with a chronic lower respiratory disease)
1/150 = 0.67% of the pop between 65 and 84 (point of ref: 1 in 107 odds of death in a vehicle crash)
1/780 = 0.13% of the pop between 40 and 64 (point of ref: 1 in 543 odds of death being run over by a vehicle)
Note that the article didn’t include the age ranges of 18 thru 40 year olds and children under 18. The most recent information I could find was from July 19, 2021 by Dr. Marty Makary (Professor at Johns Hopkins) who wrote in a WSJ op-ed piece that there have been only 335 people under 18 that have died from COVID-19, the age group which has a population of 73.1 million. That equates to 335/73.1M = .00046 % chance or 1 death in 218,208 children (a child is nearly twice as likely to die from a lightning strike 1 in 138,849). Statistically children under 18 are at zero risk of death from COVID-19.
Problem Summary: People are dying from COVID-19, let us hypothesize about how to decrease deaths.
2) Hypothesis
If a vaccine could be created, we could build herd immunity faster and less people would die.
How long would that process take to deploy a vaccine from scratch? It usually takes between 10–15 years — sometimes up to 25 years.
But, we don’t have 10–15 years and 3% of our elderly are dying from COVID right now. I would like to introduce you to Operation Warp Speed as described by then Vice President Mike Pence, head of the White House Coronavirus Task Force — “It’s amazing to think that the average development timeline for a vaccine can take 8 to 12 years. But as you heard today, we’re on track to accomplish a safe and effective coronavirus vaccine in 8 to 12 months. Before Operation Warp Speed, the fastest prior vaccine development in the United States took over four years. But as the President said earlier today, we’ve developed a gold standard vaccine in just nine months. Only in America.”
If it usually takes 8–12 years, then how was a vaccine created so quickly you ask? The following is a timeline of key moments and players along the way (pay attention to the names):
11/2/1984 Anthony Fauci assumes the director role of the National Institute of Allergy and Infectious Diseases (NIAID). One of 27 institutes that makes up the National Institute of Health (NIH).
9/14/05 French decree 2005-1181 issued declaring cooperation with China to build a BSL-4 laboratory on the Wuhan Institute of Virology campus modeled after the P4 Jean Mérieux-Inserm Laboratory in Lyons. Technology and blueprints furnished to China.
6/01/14 thru 5/31/19 — NIH funds ($666k) for the kickoff year of the project titled “Understanding the Risk of Bat Coronavirus Emergence” — Principal Investigator Peter Daszak (President Ecohealth Alliance) — describing his work in his own words. Fauci and Daszak at the Cugh 2017 conference. Peter in his own words describing how easy it is to manipulate bat Corona viruses. Dr. ZhengLi Shi (Wuhan Institute of Virology) — Pubs — Per the US State Department Fact Sheet: “The WIV (Wuhan Institute of Virology) became a focal point for international coronavirus research after the 2003 SARS outbreak and has since studied animals including mice, bats, and pangolins. WIV has a published record of conducting ‘gain-of-function’ research to engineer chimeric viruses.”
10/17/14 Moratorium on ‘gain-of-function’ research imposed — See Health and Human Services document — the NIH under Fauci “allowed it to proceed”
6/12/15 A SARS-like cluster of circulating bat coronaviruses shows potential for human emergence. North Caroline Chapel Hill paper (includes a Wuhan shoutout)
10/18/15 Development of an Ad5H3 Chimera Using the “Antigen-Capsid Incorporation” Strategy for an Alternative Vaccination Approach – paper - work supported by NIH grant
11/12/15 Nature published a paper with concern over lab-made coronavirus related to SARS — “If the virus escaped, nobody could predict the trajectory”
1/9/17 Just 11 days before leaving office, Obama re-authorizes funding for the creation of SARS biological weapons. — See White House Briefing – article
2/23/17 Maximum-security biosafety facility (in Wuhan) nears approval, sparking excitement and concern – Nature article, Scientific American article . The French state that 50 researchers will be at Wuhan for 5 years. This never happened per article, article.
1/19/18 State Department cables warned of safety issues at Wuhan lab studying bat coronaviruses – citing shortage of appropriately trained technicians - article
10/18/19 thru 10/29/19, World Military Games held at Wuhan. Possible first spread event.
11/?/19 A U.S. intelligence report identified three researchers at a Wuhan lab who sought treatment at a hospital after falling ill in November 2019 — WSJ
12/1/19 First patient manifests symptoms — Lancet study, implies infection occurred as early as two weeks prior
12/2/19 Wuhan CDC lab “moved […] to a new location near the Huanan market” (the same alleged wet (fish) market containing the contaminated bats — yet this paper says there were no bats) — NY Times
12/?/19 First known cluster of COVID-19 cases arising in Wuhan, China — per Biden Adminstration’s US Intelligence Community report
12/31/19 Wuhan Municipal Health reports 27 cases identified, 7 critical, 2 soon to be discharged
1/1/20 Huanan market closed for “sanitation”
1/3/20 Chinese National Health Commission ordered virus samples (and related information) to be destroyed if lab does not meet biosafety requirements — per US State Dept & HKT
1/5/20 Zhang, Y. (PhD, with Fudan University in Shanghai) uploaded the genome to the U.S. National Center for Biotechnology Information (NCBI) two days after receiving samples
1/7/20 Paper submitted to Nature research identifies similarity to CoVZC45 (89% nucleotide similarity & further 100% amino acid similarity in the nsp7 and E {envelope} proteins, the 100% similarity questions the theory of natural mutation) and CoVZXC21 which was sampled from bats by the Chinese People’s Liberation Army in 2018, Zhoushan China — compared to 79% similar to its namesake SARS and 50% MERS. A later study noted that the S (Spike) protein of the COVID-19 virus has a high homology (similarity, homologous) with the S protein of the SARS virus.
1/8/20 NY Times reports SARS-like Corona Virus publicly identified by Chinese researchers.
1/10/20 Chinese New Year Celebration begins — considered the largest human migration event on the planet. Estimated 5 million travelers from Wuhan (population 11 million) disseminate around China and the globe.
1/11/20 Chinese scientists (led by Yong-Zhen Zhang) submitted the genetic coding sequencing of the virus on Virological.org
1/12/20 The Shanghai laboratory where researchers published the world’s first COVID-19 genome sequence ordered to close for “rectification”
1/13/20 Professor Teresa Lambe (Lead Investigator, Oxford Vaccine Trial) and her team designed the Oxford-AstraZeneca vaccine — Per BBC documentary Panorama — The Race for a Vaccine (first 5 min)
1/20/20 First patient (man traveling from Wuhan) in the US diagnosed with COVID — King5 report
1/21/20 Realtime Polymerase Chain Reaction tests (PCR — rapid replication of DNA samples) developed by Malaysian Virologists. Primary PCR paper cited by thousands of papers since was submitted 1/21, accepted on 1/22, and published on 1/23, implying a peer review process between 4 and 28 hours.
1/23/20 CCP imposes a lockdown in Wuhan (and other regional cities in the Hubei province), setting a pattern for the rest of the world to follow. US State Dept ordered the departure of all non-emergency U.S. personnel and their family members. Moderna announces development of a vaccine. Shi (bat woman) announces birus 96.2% similar - article
1/26/20 Chinese CDC announce detection of virus at Huanan market substantiating natural origin. Also reported, a study in the Lancet suggests outbreak began elsewhere and notes patient zero has no epidemiological link from the first patient to subsequent cases, also citing 13 patients have no link to the Huanan market.
1/28/20 Travel Alert Level 4 (Do not travel) issued by the US Embassy & Consulates in China
1/29/20 Johnson & Johnson and subsidiary Janssen announce a response to develop a vaccine, White House forms the Corona Virus Task Force, statement
1/30/20 WHO director discourages travel bans — Reuters
1/31/20 Trump issues a proclamation suspending entry into the US from China, Indian researchers from Kusuma School of Biological Sciences in IIT Delhi document four additional Spike Protein sequences in comparison to SARS. These four sequences are only known to exist in the viral database in SARS-COV2, HIV gp120 (well understood by Fauci, evident in his patents), a bat corona virus discovered by Shi ZhengLi. Shi discredited the observation, but did not deny their existence. Fauci’s emails say “outlandish”. Author of the paper says he was forced to withdraw.
2/2/20 China’s Foreign Ministry Spokeswoman denounces travel bans
2/18/20 Peter Daszak makes a joint statement that COVID-19 is of natural origin, this statement effectively shut down all lab leak discussion
2/23/20 SCMP reports a published study indicates the origin outside the market.
3/4/20 Moderna granted permission to begin human trials
3/17/20 Pfizer and BioNTech announce joint development of a vaccine
3/27/20 Emergency Use Authorization Declaration
3/28/20 Therapeutic Hydroxychloroquine granted EUA as a treatment (soon to be revoked)
4/8/20 Wuhan lockdown ends
5/7/20 Pfizer begins phase 1/2 clinical trials
5/15/20 Operation Warp Speed begins — goal is to accelerate the development, manufacturing, and distribution with $18 Billion in funding
6/15/20 Hydroxychloroquine EUA revoked
7/27/20 Pfizer begins phase 2/3 clinical trials, Moderna begins phase 3
7/30/20 Johnson & Johnson begins clinical trials
9/21/20 House foreign affairs committee releases report on origins, CCP, and WHO
9/23/20 Johnson & Johnson begin phase 3
10/?/20 Human Health & Services releases non-binding recommended guidance for the EUA (Note Page 6 — Section III, Bullet 4 — the EUA is only permitted if there is “no adequate, approved, and available alternative to the product for […] treating the disease or condition.” If a cheap readily available therapeutic was shown to be “adequate” then the vaccines would not be necessary.
12/4/20 Biden discussing the vaccine states, “No, I don’t think it should be mandatory. I wouldn’t demand it to be mandatory” — Reuters
12/8/20 Margaret Keenan becomes the first in the world to receive the vaccine
12/11/20 Pfizer receives emergency use authorization
12/18/20 Moderna receives emergency use authorization
12/14/20 Vaccination begins in the US
2/27/21 Johnson & Johnson receives emergency use authorization
4/28/21 Pfizer announces development of an oral antiviral therapeutic that is a protease inhibitor. Ironically similar mode of action as Ivermectin. (Ivermectin is a medicine for humans that is effective against other viruses such as Dengue, Zika, West Nile — Paper, Paper, Paper)
6/21/21 Peter Daszak is recused from Lancet’s Covid-19 origins investigation commission.
7/19/21 UK rapid COVID Testing company Mologic announces $41 million acquisition by Sorros and Gates
7/20/21 Senate hearing on COVID-19 response; Fauci and Rand Paul on the record discussing gain-of-function research
7/21/21 CDC announces it will withdraw EUA for PCR testing 12/31/21 — clarifications made 8/2
8/2/21 House foreign affairs committee releases 3rd report on origins — zeroing in on lab leak
8/23/21 FDA excludes advisory commitee meeting and fast tracks approval Pfizer vaccine COMIRNATY. FDA requires further study on serious risks of myocarditis and pericarditis. Final reports won’t be available until 2025.
9/6/21 Details emerge (900 pages — Freedom of Information Act) connect Wuhan Institute of Virology, the NIH, and Ecohealth Alliance, Inc. inferring NIH director (Francis Collins) and NIAID director (Anthony Fauci) made untruthful public statements about supporting gain-of-function research.
9/9/21 10 months after stating he wouldn’t, Biden mandates vaccines — AP
10/5/21 Francis Collins (NIH Director) steps down — news release
Hypothesis Summary: It is possible to create an FDA approved vaccine to treat a laboratory leaked virus in 19 months if it is rushed through development, testing, and distribution (at a pace that has never been seen before). Will it work? Let us experiment.
3) Experiment
Experiment: A trial; an act or operation designed to discover some unknown truth, principle or effect, or to establish it when discovered (Webster 1828)
See here to view the vaccine testing and approval process from the CDC. Each phase expanding the pool of participants. Here is an example of the Pfizer clinical trial experiment. The CDC would vehemently object to my term “experiment” to describe the vaccine rollout, but for the purpose of this paper’s Scientific Method exercise, it is an “experiment.” Everyone who participated in the vaccine rollout under the EUA volunteered to participate in the experiment. Note: The American Public Health Association recognized the challenges in communicating these nuances in a positive light, so they wrote a paper about it and have been careful not to use the word “experiment.”
Let us ask a few questions about related past “experiments”:
Q: Has a vaccine been developed for other Coronaviruses?
A: Yes, see the study done with animal testing on SARS-CoV. “Clinical trials with SARS coronavirus vaccines have been conducted and reported to induce antibody responses and to be ‘‘safe’’ [29,30]. However, the evidence for safety is for a short period of observation.” “However, challenge of mice given any of the vaccines led to occurrence of Th2-type (allergic inflammatory response) immunopathology suggesting hypersensitivity to SARS-CoV components was induced. Caution in proceeding to application of a SARS-CoV vaccine in humans is indicated.”
Q: Have mRNA or DNA based vaccines ever been used before on a population?
A: No, this paper from 2018 heralds the prospects “The future of mRNA vaccines is therefore extremely bright” & “: mRNA vaccines have the potential for rapid, inexpensive and scalable manufacturing,” but they also note: “While preclinical studies have generated great optimism about the prospects and advantages of mRNA-based vaccines, two recent clinical reports have led to more tempered expectations. In both trials, immunogenicity was more modest in humans than was expected based on animal models, a phenomenon also observed with DNA-based vaccines, and the side effects were not trivial. We caution that these trials represent only two variations of mRNA vaccine platforms, and there may be substantial differences when the expression and immunostimulatory profiles of the vaccine are changed. Further research is needed to determine how different animal species respond to mRNA vaccine components and inflammatory signals and which pathways of immune signaling are most effective in humans.”
Q: Are there medical concerns about participants in the SARS-CoV-2 vaccine experiment?
A: Yes, this paper cites 16 different concerns. One of the primary concerns is phenomenon called Antibody-dependent enhancement, and here is a paper (And another paper) on it. “Data from the study of SARS-CoV and other respiratory viruses suggest that anti-SARS-CoV-2 antibodies could exacerbate COVID-19 through antibody-dependent enhancement (ADE). Previous respiratory syncytial virus and dengue virus vaccine studies revealed human clinical safety risks related to ADE, resulting in failed vaccine trials.” In addition, the concern in the scientific community about vaccines driving a virus is not unprecedented — paper.
So, today, a global experiment is going on in the whole of humanity. It seeks to discover the truth. Will the vaccine save lives as hypothesized? Let us review the global situation. For the purpose of this experiment, each country has adopted different approaches which will help in discovering and differentiating vaccine treatment protocols.
This paper nicely summarized the pioneering spirit of this COVID-19 vaccine experiment:
Unprecedented Many aspects of COVID-19 and subsequent vaccine development are unprecedented for a vaccine deployed for use in the general population. Some of these include the following.
1. First to use PEG (polyethylene glycol) in an injection (see text)
2. First to use mRNA vaccine technology against an infectious agent
3. First time Moderna has brought any product to market
4. First to have public health officials telling those receiving the vaccination to expect an adverse reaction
5. First to be implemented publicly with nothing more than preliminary efficacy data (see text)
6. First vaccine to make no clear claims about reducing infections, transmissibility, or deaths
7. First coronavirus vaccine ever attempted in humans
8. First injection of genetically modified polynucleotides in the general population
Worldwide* Vaccine Treatment Protocols:
* 9 other vaccines are used in less than three countries
· Oxford-AstraZeneca, adenovirus, 182 Countries
· Pfizer-BioNTech, mRNA, 129 Countries
· Moderna, mRNA 73, Countries
· Sinopharm-Beijing (BIBP), inactivated, 69 Countries
· Johnson & Johnson, adenovirus, 52 Countries
· Gamaleya (Sputnik V), adenovirus, 46 Countries
· Sinovac (CoronaVac), inactivated, 40 Countries
· CanSino (Convidecia), adenovirus, 7 Countries
· Bharat Biotech (Covaxin), inactivated, 7 Countries
Type Explanation:
· Adenovirus shell contains DNA that encodes a SARS‑CoV‑2 protein to produce only the antigen which elicits a systemic immune response
· mRNA cause cells to build the SARS-CoV-2 spike protein to stimulate an immune response
· Inactivated vaccines consist of virus particles that have been grown in culture and then are killed to lose disease producing capacity, while still stimulating an immune response. Traditional vaccine technology
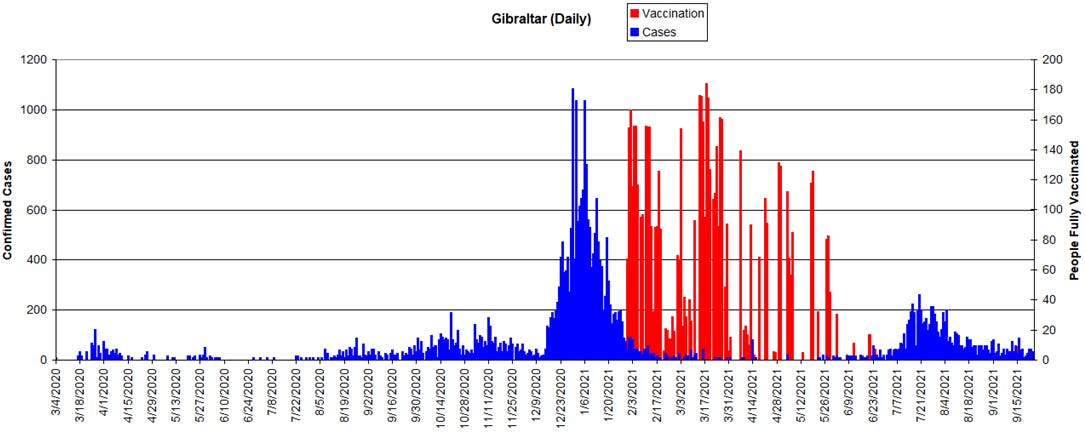
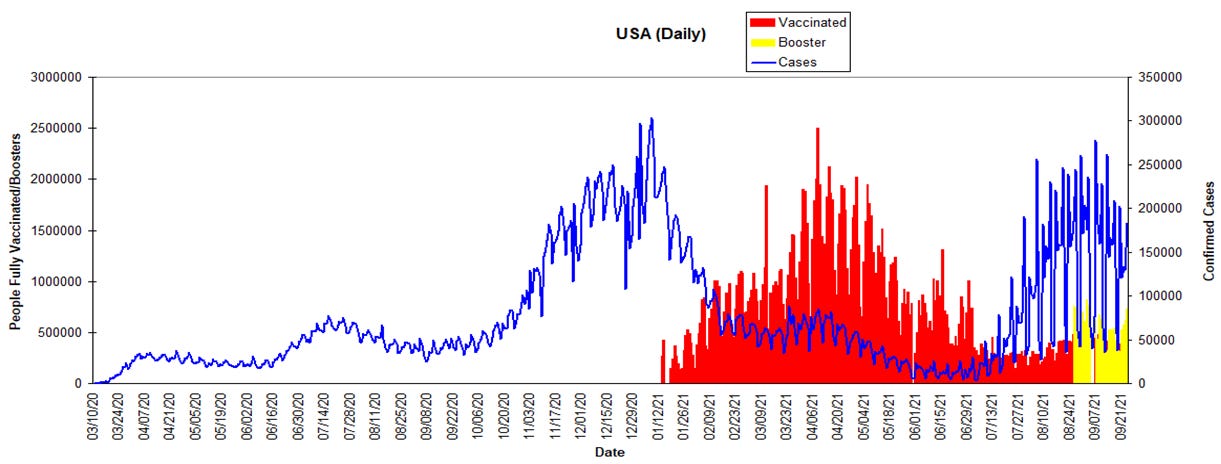
Let us now look at some data. Remember, this is an ongoing experiment, we are told that cases will rise and fall in “variant” waves. Vaccinations will increase. This was a great starting place for data, but I had a difficult time finding combined charts of vaccines and cases in a daily format, so I had to recreate them using two sources (cases, vaccinations). Another issue is that all of the vaccine charts are shown in cumulative format as they approach 100%. Note the scales are different due to population differences, and the figures are not per-capita. This is a snapshot in time. Here are a few countries farther down the vaccination path to keep an eye on over time:
Gibraltar — A tiny British Colony peninsula extending off the southern coast of Spain, Reported 100% vaccination of its 33K adult population in March. In April restrictions were reported lifted and a vaccinated utopia was declared. In July cases surged and lockdown measures were taken again.
Iceland — An isolated Island currently with a 77% rate of vaccination. They struggled with a surge in cases during late July and early August, with noting “breakthrough” cases and 60% of those hospitalized as being vaccinated. The chief epidemiologist stated that the first round of vaccinations did not lead to herd immunity and a booster program has begun. See their data here.

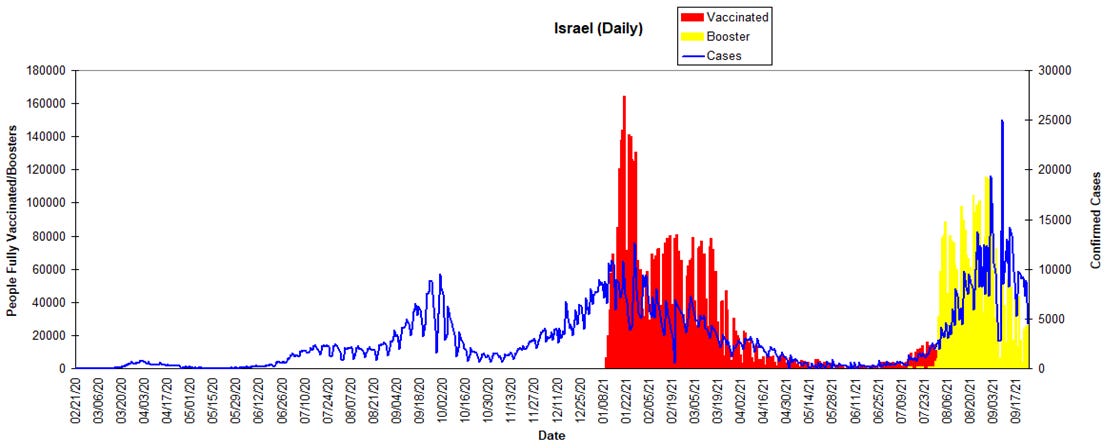
Israel — You would think the Jewish people would be wary of this level of experimentation, however there are currently 62% fully vaccinated (nearly exclusively with Pfizer). Fortune magazine reports: “Since April, Israel has fallen from 1st to 33rd in Bloomberg’s vaccine tracker of populations considered fully vaccinated. The program plateaued amid hesitancy from some in the Orthodox Jewish and Arab communities.” Philip Dormitzer, the chief scientific officer at Pfizer stated: “Early in the pandemic we established a relationship with the Israeli Ministry of Health where they used exclusively the Pfizer vaccine and then monitored it very closely, so we had a sort of laboratory where we could see the effect.” He added that Israel “immunized a very high proportion of the population very early — so it’s been a way that we can almost look ahead: What we see happening in Israel happens again in the US a couple months later.” So, what should the US be expecting as we observe Israel? Some say there is a dire warning. They began the world’s first 6 booster program in early August amid an outbreak. It was shown that the Pfizer vaccine was only 39% effective in prevention from serious illness. If an individual is not compliant with the vaccine passport system (green pass), their ability to participate in society is significantly restricted. Today, one million people haven’t received their booster, and their green pass is going to expire this Sunday. The nation’s coronavirus czar has announced that a fourth shot is expected, stating “This is our life from now on, in waves.” The most recent news reports the use of ventilators is on the rise and they are considering another lockdown as they struggle to regain control. This paper appears to have identified the mechanisms behind the breakthrough variants.
Sweden — Currently 63% are fully vaccinated. Sweden is an interesting test case because of their atypical approach to handling the pandemic — no lockdowns and optional masks. Early on they advocated for building herd immunity through natural immunity, drawing the scorn of the world. Sceptics in September 2020 were forecasting doom. One year later, cases today remain low and Sweden’s chief epidemiologist’s approach has been proven correct. It will be interesting to see how the delayed vaccination rollout plays out in future waves of cases.

United States — So how do we compare? Currently 56% are fully vaccinated. A booster program was started for the 65 and older. Despite concern and a 16–2 vote against the booster, the CDC director recently ignored the decision not to recommend boosters to anyone under the age of 65 and has recommended it to frontline workers, teachers, and nurses under 65. At least the advisory panel was assembled, unlike during the process to approve the Pfizer vaccine. Right now the CDC is in the awkward position of telling the unvaccinated to “get the vaccine” at the same time they are telling the vaccinated it doesn’t fully work, so go “get the booster”.
As we collect national data for this experiment, the CDC has made several decisions that should be noted. As of May 14, the CDC announced changes in metrics and stopped tracking “breakthrough” cases in vaccinated population unless they are hospitalized or death. Much concern was raised about the change (see letter). July 27th, the CDC announced pulling the EUA for PCR testing at the end of this year. It also should also be noted that per the CDC “people are considered fully vaccinated for COVID-19 ≥2 weeks after they have received the second dose.” This means, if you have an adverse vaccine reaction, die, or are infected with COVID sometime between your first injection and two weeks after your last injection, then your data would be recorded as “unvaccinated”. This is significant, because after reviewing the VAERs data for 2021 the overwhelming instances of onset of side effects occurred within the first 10 days.
Vermont — I did want to draw attention to one state in our union that has been doing an exceptional job at vaccination. They are sitting at 77% fully vaccinated. Unfortunately, there has been a recent record number of cases which are quick to be noted as due to the unvaccinated.

To see all as equal, here is a chart that rolls all the above countries into one chart at a per-million rate — Israel showing as the most problematic per capita:

A few other nations to keep an eye on: New Zealand recently locked down their entire country over one case. The overall risk of exposure has been low because of their ability to control entry via flights to their Islands. Australia is sitting right now at 40% fully vaccinated and with a rise in cases, they are being pressed extremely hard with lockdowns, mandates, and police state monitoring that only China could outdo. Keep an eye on El Salvador, Guatemala, Peru, and Bolivia who have just recently started providing citizens with therapeutic kits that include Ivermectin. The Indian state of Uttar Pradesh was a runaway train of cases earlier this year. They were the first sizable population to adopt wide scale dissemination of Ivermectin. The 204 million people have just a 5% vaccination rate and there are only 16 cases on a 7-day rolling average. Also note the central African countries’ low cases and low vaccination rates. Some speculate that this is due to their anti-malaria medications.
Experiment Summary: There are many different approaches to this being done by countries. A reminder, this is an ongoing experiment and the data will evolve as time unfolds — hopefully revealing new insights. Let us continue and make some observations as this vaccine experiment unfolds.
4) Observations
How does the US medical system report observations they make of vaccines? Well, positive observations are unrecorded, the system assumes the vaccines work and there are no side effects. If a negative observation must be made, per the factsheet for recipients and caregivers for all three vaccines (Moderna, Pfizer, J&J) all side effects must be reported to VAERS. VAERS is a system rolled out in 1990 that stands for the FDA/CDC Vaccine Adverse Event Reporting System (VAERS). Per this NIH paper, it is an early warning system to detect possible safety problems. In all honesty, the data in VAERS is messy. Anyone can fill out a report, of the 7% classified as “serious” it was found that “Healthcare professionals submitted 38% of reports, vaccine manufacturers 30% and patients and parents 14%”. The other challenge is that not everyone will report a side effect. The CDC funded Harvard with a million dollar grant over a three-year period and came to the conclusion that the system was being used, but was underreporting (up to one order of magnitude). There has been a surge of reports and use in the VAERS system in 2021. You can go and read reports for yourself here. Watchdog groups have been combing the data to assist in summarizing the reports. You will find one such group (read the disclaimers) and their summary here: https://openvaers.com/covid-data

The European Union has a similar system. Again, go and look for yourself. To consult the reports for COVID-19 vaccines, follow this link, then click on the letter ‘C’ and scroll down until “COVID-19”. Once you select a vaccine, then select the tab “Number of Individual Cases By Reaction Groups”. Here is a paper raising concerns.
Here is a summary of all four vaccines:

The UK also has a reporting system for observation of vaccine side effects called the Coronavirus Yellow Card Reporting Site. They publish weekly reports and you can see the latest report here.

If you would like to delve deep into the trial data: https://www.ncbi.nlm.nih.gov/sars-cov-2/
Let us not exclude from our observations the anecdotal stories of real people, not just the numbers. Every person has a story about how COVID-19 has affected their lives and many are being silenced. Here are just a few sources with numerous testimonies that you will never hear about because of censoring:
www.c19vaxreactions.com
www.1000covidstories.com
www.vaxtestimonies.org
https://thecovidworld.com/
https://thecovidblog.com/
https://covid19criticalcare.com/testimonials/
A few more simple observations:
1. The conspicuous absence of influenza in the height of the 2020–2021 flu season as reported by the CDC
2. This PowerPoint summarizes the findings from a DOD funded analysis of Medicare recipients, noting vaccine efficiency wanes over time and 2.2% death rate in breakthrough infections. In the 80% vaccinated 65 years and older population, an estimated 73% of COVID-19 cases occurred in fully vaccinated individuals.
3. A recent study out of California states: “Fully vaccinated were more likely than unvaccinated persons to be infected by variants carrying mutations associated with decreased antibody neutralization.”
Observational Summary: Observation will continue to be done for the foreseeable future. Observing the current data coming from the most vaccinated nations and states in the US points to a lack of confidence in the effectivity of the vaccines. The number and volume of associated side effects and deaths are alarming and should alone give pause for reflection by the medical community. It only took 83 cases in VAERS to raise suspicions about the rotavirus vaccination program which was terminated — paper.
5) Conclusion
In a moment I am going to try and wrap this up with my personal conclusion. I just threw months of my research into this topic at you — and if you made it this far — Yay! I imagine it is probably difficult to process all the information. I cannot fault anyone for trusting the government and the media (who I do believe have good intentions behind the desire for vaccines) as they are institutions that should be trustworthy. I also fully recognize this is counter to the narrative told to the masses for nearly two years now.
But before I share my conclusion… I want to stress that my goal with this paper is not to persuade you to arrive to our same conclusion, because you have likely already arrived at your own months ago. My goal is simply to layout the rationale behind our family’s decision not to participate in this vaccination. I believe in the coming months the pressure to conform will only increase in intensity considering the flu season approaching — the cases will rise and medical facilities will be short staffed because of mandates. Remember all those free Xbox, doughnuts, beer, Big Mac giveaways this summer? Well, those didn’t work. Now the government is swapping out the carrot for the stick. Those who choose not be vaccinated will be marginalized as reckless, dangerous, (as described by a recent columnist) gullible, logic-impaired, and stubbornly ignorant. As some of you may know we currently have family members who are facing the stark reality of losing their careers while taking a stand for individual freedom vs. the greater “common good.” This is coercion by definition. It will not be long before there will be two distinct classes of citizens with differing privileges. In the name of safety during an emergency, freedom in the US is rapidly eroding from an right to a privilege. I believe the sacrifices my family will need to make because of this choice are only just beginning.
Please know that even though we may arrive at different conclusions in this matter, we respect your decision and will continue to love you as we always have.
Conclusions based on the preponderance of evidence that I have observed:
The COVID-19 virus is a chimeric virus engineered at the Wuhan Institute of Virology from a project funded by the United States of America’s National Institute of Health (Fauci’s organization).
Flip-flop Fauci has a major conflict of interest and his leading this effort is necessary for self-preservation and controlling the narrative, akin to the fox guarding the hen house.
The NIH funded gain-of-function COVID-19 virus somehow leaked out of the BSL-4 Wuhan laboratory.
The vaccines that are being used in this pandemic are “leaky”. Meaning, they do not prevent transmission, infection, hospitalization, and only time will tell about morbidity.
A .13% chance of mortality is acceptable to me. If it wasn’t, I wouldn’t be riding in automobiles.
Mortality and hospitalizations would be even lower if supplements, prophylactic, therapeutic, and healthy lifestyle changes were encouraged (and substantially cheaper on the healthcare system).
COVID-19 vaccines have zero long-term testing on humans.
There are no plans for a control group in this vaccine experiment. Placebo groups were allegedly destroyed in the trials. Humanity is going for broke on this great gamble, it is all or nothing!
I will not inject something into my body that, if something goes wrong (such as: severe Covid vaccine side effects, or death), the maker has zero liability. The manufacturers have little incentive to ensure a safe product. The government likely won’t compensate you for damages either. CNBC
Once you get the vaccine, you can’t undo it. There is currently no antidote to tell your body to stop producing COVID-19 spike proteins. There are protocols that can be taken to minimize side effects.
The precedent that Israel is setting with boosters and cases/mortality is alarming, and could be pointing towards the manifestation of antibody dependent enhancement. Paper
In agreement with the presentations of the September 17th FDA advisory committee meeting, children don’t need protection for this virus, they need protection from this vaccine — Paper.
I fundamentally reject the reductive belief that humans are software who need annual genetic upgrades. Our genetic makeup is designed by God and should not be tampered with.
The politics of this pandemic (by both parties) is sickening. The “emergency power” grab by politicians to exploit this crisis is unprecedented. The carrot of “normalcy” is unattainable and always moving. When a politician makes a statement such as “I don’t know of any scientists or physicians who disagree”; it is not because disagreement doesn’t exist, it is because the opposition is being canceled.
As the world searches for a cure, the US’ effort to suppress the use of low-cost, safe, lifesaving therapeutics such as Ivermectin (WHO labels as essential) is criminal — meta analysis of 65 papers.
This virus will never go away. Zoonotic virus reservoirs will always exist. Paper
Natural Immunity antibodies are more robust and wider in spectrum than narrowly focused artificial vaccine induced antibodies. Paper & Article & Paper
Why would career physicians speak up and voice concern at the risk of losing their practice and livelihood? Why would vaccine victims go on social media and risk losing their account to censorship and face bullying and criticism from skeptics? Why are front line doctors, nurses, paramedics, emergency workers, first responders, and fire fighters choosing to walk away from their jobs rather than succumb to the jab (potentially 83,000 NY State)? These are examples of individuals who stand to gain nothing from these actions. What do they know that is so important to them to make these sacrifices?
Truth is capable of standing unassisted on its own two feet against assault. Censorship only raises suspicion and has never had a happy ending. Canceling, coercion and censorship seeds skepticism. The way to foster trust is to have a transparent environment where people can ask honest questions in their pursuit of truth.
We all make a cost/benefit analysis. The benefits in my eyes simply do not outweigh the risks. At the end of the day, time will be the judge. There will be heavy handed consequences imposed by man for our decision, I am certain. Those of us who oppose this vaccine need to acknowledge we are facing an opponent that is hell-bent on vaccinating the whole of humanity; they will stop at nothing and will sacrifice everything to this end. Why? This is my primary question. Also, at what point is the cost of the “cure” worse than the disease?
There you have it. I hope I have answered the question of why we are not getting this vaccine. Again, we’re not trying to convince you we’re right, I am simply communicating that we have made an informed decision.
Finally in closing, remember this edict to all who desire to satisfy curiosity and practice good science: “The important thing is not to stop questioning” quoted by Albert Einstein in LIFE magazine (2 May 1955, page 64)
POSTFACE — 10/11/21
My wife and I created this document with the intention to foster communication with friends and family. We put a lot of work into creating it. Believing it was valuable to share with others, we put it on social media. The response was very positive. By equipping people with the tools they need to have an educated conversation surrounding this topic, we hope that we will be able to collectively make a difference in our small circles of influence.
I believe self censorship is more damaging than corporate censorship. Today you can be stopped from speaking on internet based platforms, but they can’t stop you from having coffee or tea with your friends. If you can’t talk face-to-face, then make a phone call.
If you would like to personalize this document to share with your friends and family, please reach out to the email below.
We all can do our part and speak out about our reasons for “Why”.
Blessings,
J Bishop
j.bishop@tutanota.com
99% agree. But there already is a control group. It is us, the unvaccinated. And that answers the “why”. We are/will be the proof in time of the despicable and nefarious effects of this experiment.
From a Canadian police member, I thank you for putting this together. I'm sure it wasn't easy and I truly appreciate your hardwork. Only if I could memorize every word and when someone asks me why I am not getting vaccinated, I could unleash this! Thank you sir and God speed!